Not talking about the caucus winner here. Talking about a pair of grass-roots Iowans, my friends Leslie and Scott Carpenter, mental-health advocates who fit every definition of “everyday heroes.”
The parents of a schizophrenia-afflicted son brutalized by our broken treatment systems, Leslie and Scott have carried on a tireless crusade for reform that has extended more than ten years. Often they struggled in obscurity, and against indifference, until the Iowa caucuses brought the Democratic presidential candidates to their doorstep.
Their work in spreading the reform messages directly to the candidates has placed them at the center of a widening national movement to end the many atrocities of our treatment and criminal-justice systems, and the candidates are listening. I will let Leslie pick up the story here, and close by saying that these two luminous people embody the concept of “hope.”
A day after announcing the most thorough mental-healthcare reform plan of any presidential candidate, Sen. Kamala Harris was blistered in an online essay claiming her measures would hurt, not help, the seriously mentally ill. The war of words over this subject is back. Beware.
“[W]e have seen . . . a gradual increase in language that is either meaningless or destructive of meaning . . . this increasing unreliability of language parallels the increasing disintegration . . . of persons and communities.” –Wendell Berry, “Standing by Words”
“If you talk to God, you are praying; If God talks to you, you have schizophrenia. If the dead talk to you, you are a spiritualist; If you talk to the dead, you are a schizophrenic.” –Thomas Szasz, “The Second Sin”
Dr. Thomas Szaz. Credit: Jennyphotos [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)]
Szasz is dead. But Szaszism lingers on to obfuscate again.
The dark angel of opposition to social action on behalf of the mentally ill is stirring three years after his death at age 92 in 2017. Thomas Szasz’s new burst of influence, concocted from a brilliant blend of seductive yet fatally spurious rhetoric, is hardly trivial: it aims at (re)infecting political opinion about incurable brain disease, and of intimidating a hopeful new generation of advocates for mental healthcare reform.
On November 27, the heirs of Szaszian thought targeted a presidential aspirant.
In order to understand why this is important—and to learn why its importance is linked to reliable language—it is helpful to revisit the influence of a man whose artful use of words brought mental healthcare reform to a virtual standstill for more than half a century.
Thomas Szasz’s initial impact on debates over madness landed as a bombshell in 1961. His book, The Myth of Mental Illness, stun-gunned a psychiatric establishment at the peak of its popular influence. Its message found a rapturous welcome in an America primed to rebel against orthodoxy and to be persuaded that madness, that ancient dreaded specter, was nothing more than a kind of lifestyle choice, or a metaphor for commonplace distress. As for the doctors who would seek to “cure” that choice with medications and forced hospital treatment? They were nothing more than agents of authoritarian social control. Of “political tyranny,” in his words.
Szaszian thought has been quiescent for some years. Kamala Harris can tell you that it is back. Less than a week before she dropped out of the Democratic primary race on December 3, the California Senator recently announced the most far-reaching of all the Democratic candidates’ reform proposals. Her plan was immediately assailed as a threat to “the most vulnerable.”
The attack was published in the online journal Vox. Its opening paragraph declared that Harris “seems to have gone all-in on attacking the freedom, dignity, and privacy of people with mental health conditions.”
Did she really “seem to” do that? What for? The notion that a major-party presidential candidate would embrace and broadcast such sinister desires seems improbable. But this is the tao of the resistance to mental healthcare reform. Or as they presently call themselves, “the disabilities community.” In her very next sentence, the writer makes her affiliation clear: “People like me.”
Sara Luterman
The writer is Sara Luterman, an independent journalist, blogger, and self-identified victim of autism. The National Institute of Mental Health identifies autism as a “spectrum disorder” that can show a wide range and degree of symptoms. It’s also known as a “development disorder” because it can manifest in the first two years of life. Its symptoms can include difficulties in communication, restricted interests, and repetitive behaviors. Doctors believe that it is transmitted genetically and thus must be classified as disease of the brain—a mental illness. Many sufferers, it is believed, can be stabilized via medications. A more complete discussion of autism may be found here: https://www.nimh.nih.gov/health/publications/autism-spectrum-disorder/index.shtml
I am citing the consensus description of autism here because the going is about to get tricky for me, and I do not want to be misunderstood.
I don’t know Sara Luterman. I feel sympathy and respect for her as a sufferer of this affliction. I have no reason to believe that she is other than an honorable, intelligent, and courageous woman and an accomplished critical thinker.
And I strongly disagree with every argument and assertion that she makes in her essay.
My disagreements are not personal, nor do they imply any belief that her ideas are conditioned by her affliction. I take issue exclusively with her text itself.
That said:
After presuming to speak for Kamala Harris’s “extreme” intentions, Luterman widens her rhetorical authority to include the entire “disabilities community.” “Leaders in the disabilities rights community have unequivocally condemned Harris’s plan,” she asserts without documentation. On behalf of this undefined mass, she lays out several objections to Senator Harris’s specifics. She focuses on three: repealing the so-called IMD exclusion, expanding assisted outpatient treatment programs (AOT) and limiting the act known as HIPAA.
Each of these three goals is a cornerstone of the mental-healthcare reform movement. Each carries enormous social and individual implications. Each deserves to be proposed, and opposed, in responsible language. Sara Luterman, as the self-appointed spokesperson of the opposition, fails in this obligation. To itemize:
The IMD exclusion. The initials stand for Institutions for Mental Diseases. The “exclusion” refers to a Medicare provision that prohibits funding for care facilities with more than sixteen beds. The Mental Illness Policy Organization has reported that as of 2005, the most recent reporting year, only seventeen beds existed for every 100,000 potential patients, a drastic shrinkage from 340 per 100,000 in 1955. The total estimated shortfall is more than 120,000. This, in the opinion of many advocates, amounts to “the federally mandated discrimination against the seriously mentally ill.”
The consequences of this shortfall play out regularly in national news coverage: the staggering numbers of mentally ill people at large on the municipal streets, the dumping of this same luckless population into our overcrowded jails and prisons. Some 378,000 incarcerated persons have severe mental illness. An increase in psychiatric beds would logically enable expanded care centers to ease the glut in these arenas of human hopelessness. Senator Harris would double the number of psychiatric treatment beds. This would amount to a maximum of thirty-two beds per facility.
Yet Luterman ignores the clear humanity of such an outcome. For her, this modest increase in the number of beds can lead to only one monstrous consequence: the return of the insane asylum.
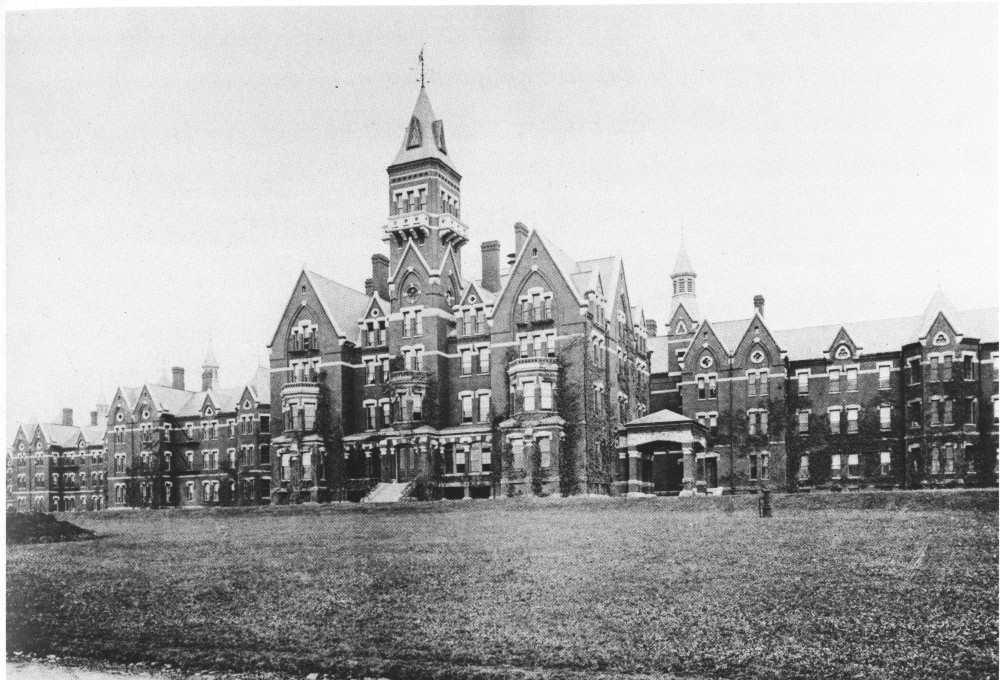
The insane asylum. Few phrases are burned more deeply into the national consciousness; few bear more sinister imagery: brooding colossal piles of brick and granite, whose choked corridors echo with the wails of the beaten, the chained, the starved, the raped, the socially damned. The images derive from such now-extinct hell-holes as the Trans Allegheny Lunatic Asylum, with its 2400 patients crammed into space intended for 250. Or Greystone Park, with 1189 patients in its 800-capacity confines. Or Danvers Asylum, with 2000 patients stuffed into space designed for 500. These are among the proto-haunted houses of our nightmares.
Danvers State Hospital, c. 1893
Is this what Luterman means by “insane asylums”? She does not bother to say. She neither defines nor delimits what she means. She simply hangs the term out there and allows the reader to interpret the semiotic. And to let the Harris plan’s 32-bed maximum swell to gothic imaginary dimensions.
The reader might better ask: why is such a consequence inevitable? It assumes we have learned nothing from the disastrous epoch of the Big Asylum. The conservative social/political critic Norman Ornstein—whose mentally ill son Matthew died in 2015—offers what strikes me as a far more clear-eyed, less apocalyptic prospectus. He supports an increase in the number of psychiatric beds. He would populate their still-scarce number with the most abject cases and build in strong oversight requirements to forestall decay and abuse.
Ornstein writes,
“Make it clear, that you are concerned about those people with the most serious mental illnesses who have no insight into their diseases, will not accept treatment, and are often captives to their delusions. Anosognosia [the illness-induced lack of insight] is a real phenomenon for a substantial portion of those with serious mental illnesses; it is not a choice but an integral part of their brain diseases.”
DJ Jaffe
Closely aligned with increasing beds is Senator Harris’s embrace of more funding for AOT. DJ Jaffe of the Mental Illness Policy Organization makes the common-sense argument that competent outpatient treatment is a lifeline to those who wander in a haze of cognitive bewilderment on city streets and risk committing an irrational act that will land them behind bars. But to Luterman, AOT offers nothing of the sort. It is merely “paternalistic,” and a mechanism for “forcible” medication and treatment, a concept loathed by the disabilities community.
Here is another view, from a member of the selfsame “disabilities community” that Luterman claims to speak for. Eric Smith is a young, afflicted Texan who is making a name for himself as a rising speaker and writer for reform causes. A few days ago, Eric responded to the controversy thusly:
“Those who fight against strong AOT programs and better access to psychiatric beds are fighting for my right as an individual diagnosed with serious mental illness to be a victim of the demons that own every part of who I was before a psych bed and AOT saved my life.”
“Forcible,” “forced,” and “involuntary” are the most pre-emptively punishing words in the anti-treatment arsenal. They trace directly to Szasz, who founded his entire crusade of resistance to any form of treatment on the argument. Szasz saw government intervention as an instrument of authoritarian control: Psychiatry is “an arm of the coercive apparatus of the state,” he wrote, and thus “All of medicine threatens to become transformed from personal therapy into political tyranny.” Involuntary mental hospitalization was like slavery. And: “The dogmatic view that mental diseases are brain diseases, treatable with chemicals, dehumanizes the patients.”
It is important to contemplate the fact that Szasz formed common cause with that notably clear-thinking L. Ron Hubbard, the founder of Scientology. And that his ideas caught the attention of the American Civil Liberties Union, which exalted his view that forced medication and treatment of a person in psychosis violated the person’s civil rights. That alliance irradiated social policy. In 1975, the Supreme Court ruled, in effect, that it is unconstitutional to commit for treatment an individual who is not (imminently) dangerous. The test for imminent danger was not specified.
When microcomputer breakthroughs in the mid-1980s produced evidence that brain diseases indeed existed—detectable as tiny lesions caused by the cocktail of flawed genes in schizophrenia patients—Szasz was not moved: “The evidence is not scientifically compelling.” Fake news, so to speak.
These of course are classic Libertarian views; and Szasz, a prewar immigrant from a nation (Hungary) situated between two totalitarian powers—Russia and Germany—bore an understandable aversion to totalitarian thought of any stripe. Ironic, then, that his own ideas bore the mark of absolutism. They allowed no compromise, no modification, no re-interpretation in the light of new evidence. Just unconditional surrender. His inheritors in time present show similar rigidity, though their attempts at aphorism lack the master’s panache. “It is not an America I would like to live in,” is a typical Lutermanian turn of phrase.
This brings us to (3), the act known as HIPAA.
The initials stand for the Health Insurance Portability and Accountability Act. HIPAA, enacted by Congress in 1996, seeks to assure the privacy of a patient’s medical records without the patient’s consent.
In theory, such protection is praiseworthy. In practice, HIPAA laws seal out not only snooping insurance providers, journalists, and potential employers, but also close relatives frantic for information on their loved one’s diagnosis, condition, treatment plan, medication, and degree of stability. “Normal” patients may volunteer such information to their families. Patients in psychosis generally lack capability for rational consent of any kind.
Leslie Carpenter, the Iowa advocate who presented her colleagues’ reform plan to Senator Harris, has explained HIPAA’s deficiencies in some detail:
“First, it is a concern about the lack of two-way communication that helps the family to more actively support the loved one who is sick. Providers hide behind HIPAA to avoid talking with family, and this limits active collaboration that allows the family to tell the providers about the patient’s actual symptoms and function.
“Second, some families take home a sick loved one without even knowing the diagnosis, the medications needed and how vital they are, what side effects to watch for, and when to schedule follow up-appointments. Because of HIPAA restrictions, they can’t actively help get the sick loved one to appointments and to take their medications.
“Third, sometimes/often, loved ones are discharged before being stabilized: while they are actively suicidal or having thoughts of hurting others. Because of HIPAA, no one informs the family. This puts the person and all those near the person at risk.”
Common sense—and the Harris plan—would amend HIPAA so that it permits family members to receive information of this kind while screening out others. This is not enough for Luterman and the disabilities community. For her, and presumably for them, HIPAA compromises would be one thing and one thing only: “extreme.” “Harris would allow health care professionals to disregard the consent of their patients if they happen to think [sic] doing so is important,” she writes. No acknowledgment of the complexities laid out by Leslie Carpenter.
My focus so far has been on three important reform plans that Senator Harris proposes and Luterman attacks. Yet the damage that Luterman seeks to effect is more general. Her Vox essay is weighted with grievance that does not bear close examination. Specifically, she raises the oldest, most pernicious complaint in the Szaszian followers’ playbook: that the seriously mentally ill do not have veto power over professional efforts to help them in times of crisis. (Recall: “Forcible,” “forced,” and “involuntary.” Recall psychiatry as “an arm of the coercive apparatus of the state”).
Recall these pronouncements. And then recall the towering, historically unique conundrum that serious mental illness embodies:
Serious mental illness is different. It is categorically unique. It has no analogs—not in human behavior, not in medicine, not in law, not in the sphere of ethics, not in its capacity to trigger heartbreak and catastrophe and dread.
Serious mental illness removes volition.
Serious mental illness makes it impossible for all but a few of its victims to arbitrate whether they will allow treatment because it nullifies the arbitrating mechanism. To paraphrase Danny DeVito in Heist: “That’s why they call it mental illness.”
All of that said: I, and many other advocates for reform (I can’t speculate on how many) recognize the many, many variables—and the contradictions—that are baked into this most diabolical of afflictions. I—we—I—recognize that so much remains a mystery. That medications, our best hope for surcease until a cure is found, do not work equally well from one patient to the next. (Yet they generally do work in their task of temporary stabilization.) I recognize, and have written about, the monstrous legacy of fraud and profiteering in Big Pharma. I recognize that at least some care centers, and some care-givers, are incompetent, doing more harm than good. I recognize, I recognize, I recognize.
Yet even in the depths of grief I have often endured since the suicide of my son Kevin, who was not helped by any of the structures erected to reclaim him and his fellow-sufferers—even in these depths—I pull myself back by clinging to these verities:
This is the hand we have been dealt.
Our efforts are far from perfect, and sometimes calamitous.
We must keep groping through the fog until we or our descendants stumble into the light.
This is our dharma. Our sacred duty.
And to those who try to bury our reform ideas in waves of false rhetoric—under extreme! And dangers! And rights! And shame!
To those people, this must be our sole and all-encompassing response:
In one breathtaking stroke, Kamala Harris has just widened the contours of presidential campaign history and thrown light into the darkest corridors of shameful human suffering.
On Monday, Harris affirmed that America is in the throes of a mental healthcare crisis. And she backed up her ringing assertion by adopting all the major goals of advocates for enlightened mental healthcare and fairness in our nation’s policies and practices. While several of her rivals for the Democratic presidential nomination have put forth their own reform proposals, none matches the sweep of the Harris plan, and none has triggered such rejoicing in the ranks of reform advocates.
In the words of the premier advocate-warrior DJ Jaffe: “Wow! Wow!” Jaffe added that the Harris plan embraced “everything we’ve been looking for to help [the] seriously mentally ill.”
With these gestures, Harris has frontally attacked a century’s worth of neglect, denial, obfuscation, and wasted spending that define the country’s medieval approach to its most helpless citizens.
Among her plan’s many, desperately needed virtues:
The Harris plan reinvigorates the concept of “justice” in dealing with the mentally ill; yet it implies a range of practical economic benefits as well. Her agenda attacks the widening cone of unnecessary social cost and structural blight that proceeds from the stricken individual through the community, the city, the rural landscape, and our vast failed archipelago.
In calling for a doubling of the nation’s psychiatric beds, for example, Harris opens a path to significant reduction of taxpayer money spent on the glut of afflicted people behind bars: Each year more than 2 million people with serious mental illness are thrown in jail, often because care centers have no room. Incarcerating an inmate with mental illness costs $31,000 annually, while community mental health services cost about $10,000.
Harris’s recommendations are protean. They contemplate the needs of psychically damaged veterans; telemedicine as a resource in under-served rural communities; the elimination of foolish laws that prevent family members from learning the state of a relative in hospital care; an increase in crisis-intervention teams; criminal-justice diversion for people in psychoses arrested for a crime; education for a judiciary too often clueless as to the nature of mental illness, and “Medicare-for-all” coverage for the mentally ill.
And it calls for the abolishment of the evil known as solitary confinement. Other Democrats have attacked this scourge as well, though that is hardly a discredit. Solitary confinement cannot be excoriated too many times.
The Harris plan is not exactly sailing in calm political waters, of course. The cynicism and bad faith that now besmirch our civic discourse might well capsize this vessel of reforms. Some pundits will almost surely write it off as a desperation gesture from a candidate struggling to gain traction in the polls–or as a cosmetic ploy to soften Harris’s residual image as a remorseless prosecutor.
Such dismissal would be as shameful–as borderline-decadent–as is the present state of mental healthcare itself. Kamala Harris’s proposed reforms are what they are, without reference to the candidate. They cry out to be lifted up from the ruck of conventional campaign promises and examined (and re-examined, and debated, and circulated“, and published) on their own merits.
And they are something beyond themselves, as well: they are a blazing collective affirmation of the power of witness: persistent, retail, on-the-ground political advocacy. To the politics of personal persuasion and response, if you like.
Leslie Carpenter and Kamala Harris Photo Courtesy Leslie Carpenter
Virtually every Democratic candidate who has spoken up about mental health-care reform has been educated on the soil of Iowa, face-to-face, by the phenomenal team of Leslie and Scott Carpenter. They and their fellow advocates–my friends and models of informed passion and persistence–are living testaments to the ideal of Making a Difference. Most of these people have struggled for years, in small groups, in letters and emails to the powerful, and against fatigue and hopelessness. Nearly every one of them is closely related to a victim of serious mental illness.
Now, just maybe, is their moment.
I am NOT homeless!
I have a home!
My home is the United States of America!
James Mark Rippee
James Mark Rippee after his motorcycle accident June 1987
Listen to the words above. Say them aloud. And try not to feel stirred. Angry. Transformed. Try not to feel inspired to stop what you’re doing and throw your energies into a cause that is becoming a national movement.
Maybe you can do this. Maybe you can hear those words and remain unmoved. Maybe you can hear them and shrug and turn back to the duties of your day.
I cannot. I can’t stop hearing them. I hear those words as fierce poetry. More to the point, I hear them as a manifesto, one that should take its place among the great declarations that have defined our nation and our obligations toward it, and its most maimed and outcast citizens.
I hear it delivered with the same patriotic pitch as “Give Me Liberty Or Give Me Death.” “The Better Angels of Our Nature.” “Ask Not What Your Country Can Do for You; Ask What You Can Do for Your Country.” “We Can Do Better.”
The words are the more compelling in that they were uttered–on Wednesday, October 2–by a man so grievously crushed by brain injury, schizophrenia, blindness, broken bones, and more than twelve years struggling for life on the streets that one hardly imagines him capable of speaking a coherent sentence, much less this burst of eloquence.
And this is exactly the fundamental barrier that inhibits people and political bodies from doing more to rescue the mentally ill who cling to existence in desperate circumstances–to rescue the mentally ill, period. Consciously or unconsciously, they are seen as not fully human. Monsters. Half-sentient beings who “don’t even know they’re living that way; but perhaps they like living that way,” in the considered analysis of the current president of the United States.
These are essential reasons why, as it has been said, no one cares about crazy people.
The man who spoke this manifesto is James Mark Rippee of Vacaville, California. You know Mark’s story if you have followed several entries in my blog. Nearly killed in a collision while riding his motorcycle in June 1987 that blinded him and left parts of his brain in an alfalfa field; prohibited by his distraught father (who died of a stroke a few years later) from commitment to an institution; endurer of nearly fifty operations to remove abscesses from his brain; cared for by his sisters Linda and CJ until his violent psychotic episodes made him a danger in the household; a street refugee for a dozen years and counting as the two sisters have petitioned his case to the blind eyes and deaf ears of numerous agencies and levels of government.
Mark Rippee
The sisters’ goal is simple, and reasonable to anyone with a bit more compassion than God gave a goose, or a Solano County pol: to secure conservatorship for Mark a measure that allows county public health officials to steer mentally ill and homeless people toward housing and medical treatment without their consent.
(The requirement of consent has, for more than half a century, stood as a vexed impediment to providing medical and psychiatric care for people in psychosis who refuse to admit that they need it. Designed to protect such victims from fraud and predators, “consent” in practice has blocked emergency help victims of psychosis who will not or cannot admit they are ill.)
Linda and CJ have fought across two decades for their brother’s reclamation–for some mechanism of policy that would remove him from the streets where he has been routinely ridiculed, robbed, and beaten up–and into some safe place; some room; some bed; some sanctuary where doctors could nourish him, salve his wounds, give him medications to tame the psychotic demons inside him.
No agency in the state of California is interested. California harbors half the homeless people in the United States, and so the violate humanity of Mark Rippee has not sunk in. He is just another statistic. The Solano County Board of Supervisors has long since grown tired of the sisters’ petitions and their pleading. They have stopped pretending to care. They say that Mark Rippee is not their responsibility. Linda and CJ believe otherwise. But they have lacked the money and the access to public attention to make their case.
Wavelets of sympathy, gestures toward “doing something,” arise and fade. And Mark Rippee edges ever-closer to a sordid death on the streets of Vacaville.
Ironically–and ironies glut the world of mental illness–it has taken another vehicle accident to galvanize a fresh groundswell of support for Mark Rippee’s cause.
On the evening of September 14, as Mark wandered blindly along Monte Vista Avenue in Vacaville, he stumbled into traffic and was hit by a car. (Until then, he miraculously had eluded such a mishap during his years on the streets.) His head struck the concrete pavement, re-opening the abscess behind one of his eye sockets. The pain evidently was so intense that this time Mark agreed to be hospitalized.
At this writing, October 4, Mark remains in a Vacaville hospital. His sister Linda has been with him. (CJ’s mobility has been limited by illness.)
It was a nurse’s question about Mark’s residency, and Linda’s response to it, that prompted Mark’s burst of eloquence.
“The nurse came in [to Mark’s room] and questioned me about what equipment or help he has at home,” Linda told me by email. “I said without thinking, ‘He is homeless.’ And Mark loudly said, ‘I am NOT homeless. My home is the United States of America!'”
Linda added, “If only he knew how he was abandoned by his own country.”
Mark Rippee’s abandonment; at least, his invisibility, may be near an end. While it is true that every level of American governance has ignored him or brushed him aside so far, a grass-roots movement–tiny in numbers yet explosive in its sudden presence and growth–has sprung up in his behalf.
On September 30, a Solano Community College student named Kacie Hill created a Facebook page, “Mark of Vacaville.” . By Friday afternoon, it had attracted 1,300 members. A young Vacaville man, Jaden Ghent, began printing T-shirts in various colors, with images of Mark and the text of his manifesto. A rally on his behalf is being planned for Sacramento, the state capital.
If the Mark Rippee story is in fact arriving, it will not be a moment too soon. He is 56 now, and obviously in terrible health. If he is not rescued from the streets soon, especially with winter approaching, his life may end soon.
I have been convinced for two years–since discovering his plight upon commencing this blog–that Mark’s saga is of national significance; that this tragic, deformed man might well serve as a living symbol of so much that is deformed in our systems of mental health care. In these two years I have contacted political figures (including the Solano County Board of Supervisors), media watchdogs, and mental health advocates on his behalf. The advocates have shown interest but none has had an idea for how to break through. The rest have remained stonily silent.
But last Wednesday, with one impassioned, eloquent outburst, Mark Rippee may have done the trick himself. However improbably, he has risen up from his tortured silence to declare himself a man. Whose home is the United States of America.
And people–ordinary grass-roots people, if not (yet) those who represent the United States of America–listened.
And the silent, suffering, frequently incoherent James Mark Rippee of Vacaville, California, may yet transcend his victimhood and become the standard-bearer of reclamation that we have all been looking for.
Two mobilizations of historic enlightened reform are abruptly converging in American politics and policy. Their aims are intertwined: to bulldoze and rebuild our blighted structures of criminal justice, and to reclaim our dispossessed mentally ill brothers and sisters from the hellscape of danger, pain, and early death that the blight of justice confers on them. And the economic drain that it exacts from all of us.
The symbiotic forces are (1) the elite tier of progressive candidates for the 2020 presidential election, and (2) the sleeves-up cadre of activists working at Ground Zero who toil because they daily confront serious mental illness up close, and witness its effects for what they are: cancers upon our societal health and sense of decency.
(The first of two parts)
At first glance, justice and mental-healthcare reform may seem but a marginal sliver of all the issues pressing in on America in the 2020 elections. (The physical salvation of the planet comes to mind, and abolishing the immigrant gulags at our southern border.)
This is a distorted, damaging perception, made more dangerous because the crisis is so easily concealed. It can sometimes seem as though insanity and incarceration are like two undersea predators, their tentacles wrapped around each other in a death-struggle of futility. The quality of courts, jails, and prisons has been weakened by years of tending people who should be under psychiatric care. The essentially helpless 11.2 million seriously mentally ill population in turn is vulnerable to suffocation in the folds of feckless court rulings and inhumane treatment behind bars, including deprivation of essential meds and the beckoning maw of solitary confinement (about which more—much more—later.) The one in five adults with less chronic afflictions—nearly 47 million—are within range of the tentacles as well.
Yet that perception, or lack of perception, prevails. It prevails because to open our eyes to the full truth of these abominations is to risk scorching the soul. “I’ll do what little I can in writing,” lamented the great James Agee in another, and again oddly similar context some 75 years ago. “Only it will be very little. I’m not capable of it; and if I were, you would not go near it at all. For if you did, you would hardly bear to live.”
Thus we banish the ghastly effects from our attention as “normal” Americans, until it is too late. The entwined crises strike quickly, and from nowhere, and spread ruin: in households and communities (black and poor ones especially), in the workplace, in public places, in our economic state, and in the less tangible spheres of our collective optimism, hope, and peace of mind.
America has needed an “intervention” for more than two centuries. Intervention seems, at last, to be on its way.
The most ambitious manifestos, in my unscientific reckoning, were issued within the last ten days by Senators Bernie Sanders and Elizabeth Warren and South Bend, Indiana Mayor Peter Buttigieg. Nearly as powerful were the earlier justice reform announcements of Cory Booker, Amy Klobuchar, and Julian Castro. Joe Biden and Kamala Harris submitted strong, if not notably comprehensive, reform ideas.
This ranking hierarchy is not as fixed as the tiers might imply. The eight plans are far more significant for their overlapping reform goals they stress than for their differences.
Elizabeth Warren
Slashing into federal prison glut is high on most lists. Sanders, Warren and Buttigieg unveiled proposals that would cut into mass-incarceration, each by roughly 50 percent: by reducing long sentences, ending the “cash bail” system that pauperizes poor families of those arrested, tightening up on police oversight, legalizing marijuana, and abolishing private prisons. Sanders’s document, at 6000 words, is by far the most minutely detailed. Warren would go after policies that “criminalize” homelessness, poverty, and mental health problems (critically, she has not elaborated on this last). Booker would scale back inmate numbers via a clemency program that would free many elderly inmates under the theory that criminals “age out” of their impulses to commit violent crimes. Klobuchar also embraces clemency via a restructured reform plan and would modify the “tough-on-crime” stances she held as a prosecutor in Minnesota.
Julián Castro
Castro’s vision is likewise far-ranging, but he places special emphasis upon overhauling violent and clueless behavior of policemen. He wants to curb the use of force, end stop-and-frisk, holding police more accountable for misconduct, and restoring trust among police and the communities they are sworn to protect.
As for Biden and Harris, their reform plans are similarly comprehensive and replicate the bold ideas of their rivals as listed above. Both candidates—and to some extent Klobuchar as well—are preoccupied with freeing themselves from the taint of the “tough-on-crime” stances that they adopted in the mid-1990s.
That is my personal survey, unfairly truncated perhaps, of the generally ground-breaking flurry of criminal-justice reform ideas released by eight of the leading progressive presidential candidates.
An obvious but important caveat: none of these audacious ideas will tap-dance its way into law or policy should its sponsor get elected. (The proto-autocrat decrees of our current incumbent might lull some into that assumption.) A new chief executive will need to inspire the House and Senate to a pitch of pro-active fervor not seen since the First Hundred Days of Franklin D. Roosevelt’s presidency when the New Deal took form in a blizzard of “relief, recovery, and reform.” For our present stumbling and divided Congress to suddenly sprout capes, masks, and flippers and get busy cleaning out the present rot may seem a stretch. Yet things can happen quickly, as the last midterms showed, and a whiff of activism does linger in the air.
With all this in mind, let us turn to the symbiotic manifesto that has arisen from those ordinary heroes at Ground Zero: “Grassroots 2020: A 5-Part Plan for Mental Illness SMI.”
Grassroots: 2020 has been personally distributed to visiting Democratic candidates or mailed to their offices by Leslie and Scott Carpenter of Council Bluffs, Iowa. The Carpenters’ tireless work has helped join the reformist trajectories of these politicians and the people.
I lay it out below with minimal editing, in summary form. You will note that each part of the plan delineates action that a president can undertake, sometimes independently of Congress. And unlike the candidates’ ideas above, Grassroots: 2020 addresses justice-reform issues (incarceration-trimming, for example) only incidentally. It focuses on existing rules, many of them arcane to the non-specialist, that nonetheless have caused decades of frustration and despair for those struggling to reclaim their afflicted loved ones from a decayed system:
A FIVE-PART PLAN TO ADDRESS SERIOUS MENTAL ILLNESS (SMI) 2020 PRESIDENTIAL CANDIDATES. PLEASE ADDRESS THESE TOPICS IN YOUR CAMPAIGN APPEARANCES AND DEBATES:
1. RECLASSIFY SERIOUS MENTAL ILLNESS (SMI) FROM A BEHAVIORAL CONDITION TO WHAT IT IS – A NEUROLOGICAL MEDICAL CONDITION
WHY RECLASSIFICATION IS IMPORTANT:
Re-classification will unlock more research funding and help eliminate discrimination in treatment, insurance reimbursement, and the perception of SMI as a “behavioral” condition. SMI is a human rights issue. The National Institutes of Mental Health ranks SMI among the top 15 causes of disability worldwide with an average lifespan reduction of 28 years.
PRESIDENTIAL ACTION:
• Create a cabinet position exclusively focused on SMI. • Push for Congressional appropriations to include schizophrenia in a CDC2 program that collects data on the prevalence and risk factors of neurological conditions in the U.S. population.
2. REFORM THE HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA)3
WHY HIPAA REFORM IS IMPORTANT
Overly strict HIPAA laws make it extremely difficult for families and caregivers to partner in the treatment of their loved ones, resulting in important life-saving medical information gaps. By eliminating this barrier, family support will be strengthened, reducing the chance of relapse, homelessness, imprisonment, and death.
PRESIDENTIAL ACTION:
Work with legislators to change HIPAA law to ensure mental health professionals are legally permitted to share and receive critical diagnostic criteria and treatment information with/from parents or caregivers of SMI.
3. REPEAL MEDICAID’S INSTITUTES FOR MENTAL DISEASE EXCLUSION (IMD).
WHY IMD REPEAL IS IMPORTANT:
The Medicaid IMD Exclusion prohibits Medicaid payments to states for those receiving psychiatric care in facilities with more than 16 beds for those in the 21-65 age group. This demographic represents the majority of SMI cases. Repeal of the IMD Exclusion will increase the availability of acute care, inpatient psychiatric beds. The IMD exclusion not only discriminates against those suffering from neurological brain disorders, it’s a leading cause of our national psychiatric hospital bed shortage.
PRESIDENTIAL ACTION:
• Work with legislators to repeal the IMD exclusion.
4. PROVIDE A FULL CONTINUUM OF CARE FOR THOSE WITH SMI
WHY A FULL CONTINUUM OF CARE IS IMPORTANT:
A continuum of care insures that SMI patients receive early intervention at all stages of their illnesses, long-term care when needed, and follow-up treatment (medications and therapies) when they’re released. Providing a continuum of care reduces: incarcerations, emergency rooms visits, homelessness, and death. A continuum of care provides life-time management that permits a patient to move without penalty from one level of care to another as needed.
PRESIDENTIAL ACTION:
• Create federal incentives to states which are addressing a full array of inpatient, outpatient, and supportive housing care.
5. DECRIMINALIZE SERIOUS MENTAL ILLNESS (SMI)
WHY DECRIMINALIZATION OF SMI IS IMPORTANT:
People suffering with other neurological conditions like Alzheimer’s and dementia can get treatment promptly without being kicked out of their homes to wander the streets until they are arrested and put in jail or prison rather than a hospital. Serious mental illness is the only disease where the doors to treatment are shut unless a crime is committed. This is pure and simple discrimination with the disastrous results we see in our country today — homelessness, incarceration, the disintegration of families, and death.
PRESIDENTIAL ACTION:
• Work with legislators to change “must be a danger to self or others” criteria. • Work with legislators to change involuntary commitment criteria, alleviating the subjective nature of “gravely disabled” and redefining it in objective terms based on scientific medical need for treatment. Psychosis, like a stroke, is a traumatic brain injury and needs immediate treatment for the best outcome.
Bernie Sanders
Returning to the candidates’ manifestos, I have omitted two demands that show up in most of them, yet are given no more than lip-service by none except Bernie Sanders: abolishing capital punishment and solitary confinement. Both are urgent. Deciding which is the most urgent depends, I guess, upon the morbid calculation of whether continued existence in the “hole,” with its barbaric history of destroying human personality, is worth the torture. I have felt my way to an agonizing decision. In my next blog I will urge the candidates to meditate on solitary confinement for exactly what it is, and to treat it as primary target for abolishment.
QUINCY — Pulitzer Prize winning author and Hannibal, Mo., native Ron Powers will speak in Quincy next month in support of the Transitions Foundation.
The foundation will host “An Evening with Pultizer Prize Winning Author, Ron Powers” at 8 p.m. April 26 at the Oakley-Lindsay Center, where he will speak about his writing career, as well as the challenges and obligations of exploring family tragedy.
In 2017, Powers released “No One Cares About Crazy People: The Chaos and Heartbreak of Mental Health in America.” It describes the ravages of schizophrenia, which afflicted his two sons and triggered the suicide of his younger son Kevin in 2005. The book offers a critique of the mental health systems in the nation.
“I think it will be an interesting evening for people in our area who know he had grown up in the Hannibal area, as well as people who have an interest in history and his writing about the six men who planted the flag on Iwo Jima and people who have an interest in mental health and the status of mental health services in our country,” said Barb Baker Chapin, director of development at Transitions of Western Illinois.
Powers is the co-author of “Flags of Our Fathers” and “True Compass,” which were both number one New York Times hardcover nonfiction bestsellers. His biography of Mark Twain, “Mark Twain: A Life” also was a New York Times bestseller and a finalist for the 2005 National Book Critics Circle Award.
He was awarded the Pulitzer Prize for his critical writing about television for the Chicago Sun-Times in 1972. He also won an Emmy Award in 1985 for his commentaries on “CBS News Sunday Morning with Charles Kuralt.”
The event is sponsored by The Herald-Whig, WGEM, the Blessing Health System and Knapheide Manufacturing.
All proceeds from the event will support mental health services at Transitions.
Tickets for the event are available at the Quincy Community Theatre Box Office in the Oakley-Lindsay Center, which can be reached at 217-222-3209.
Tickets also can be bought online at 1qct.org, by clicking on “upcoming events.”
A limited number of tickets are available at $75 per person for a meet and greet with Powers from 6:30 to 7:30 p.m. The event includes a social hour with hors d’oeuvres, a complimentary copy of “Flags of Our Fathers,” and opportunity to meet Powers during a book signing and preferred seating for Powers’ talk.
Tickets for the talk are $25 for preferred seating and $15 for general admission.
Copies of several of his books will be available for purchase at the event.
I was honored to deliver this talk on November 4 at Austin, at the annual meeting of the American Association of Medical Colleges. AAMC is a 142-year-old organization dedicated to improving American health care through educational initiatives and state-of-the-art medical research. My invitation signaled that the AAMC has recognized mental healthcare as an essential part of their outreach.
I feel grateful to the distinguished outgoing president of AAMC, Darrell G. Kirch, MD, for his warm introduction, and to Stacia Gueriguian of the AAMC for her superb stewardship of the technical production. If you find the talk useful, I urge you to repost it on the web, and perhaps to recommend it to a university, public-school system, or community-access channel in your area.